Trust Admits Liability and Settlement Details
The hospital trust admitted liability for medical negligence. The experts agreed that the patient met the criteria for thrombolysis and/or thrombectomy at the time of first presentation, and that the failure to activate the stroke pathway constituted a breach of duty that directly caused or materially worsened the extent of the brain damage.
A substantial settlement was agreed to compensate the patient for pain and suffering, past and future care costs, loss of earnings and earning capacity, adapted accommodation, specialist equipment, private therapies, psychological support and assistance with daily living. The package ensures financial security for lifelong needs arising from the medical negligence.
While the compensation addresses practical and financial requirements, the family stresses that no amount can restore the independence and quality of life lost due to medical negligence. The settlement reflects the severity of the preventable harm and the lifelong consequences of the delayed stroke treatment.
Long-Term Impact After Medical Negligence
The patient now lives with permanent severe disability caused by medical negligence. Right-sided hemiplegia means no functional use of the right arm or leg, expressive aphasia limits communication to yes/no responses and gestures, dysphagia requires modified diet and thickened fluids to prevent aspiration, and cognitive impairment affects memory, concentration and decision-making.
The medical negligence has also caused significant psychological harm to the patient and family. The patient experiences frustration, depression and loss of self-esteem due to the sudden, permanent dependence. The family provides much of the emotional and practical support while dealing with their own grief and stress caused by the preventable outcome.
The patient and family have chosen to share the case to raise awareness of the critical time window in stroke care. They hope other patients receive immediate recognition and treatment of stroke symptoms so medical negligence does not cause similar catastrophic, avoidable disability.
Lessons from the Preventable Stroke Outcome
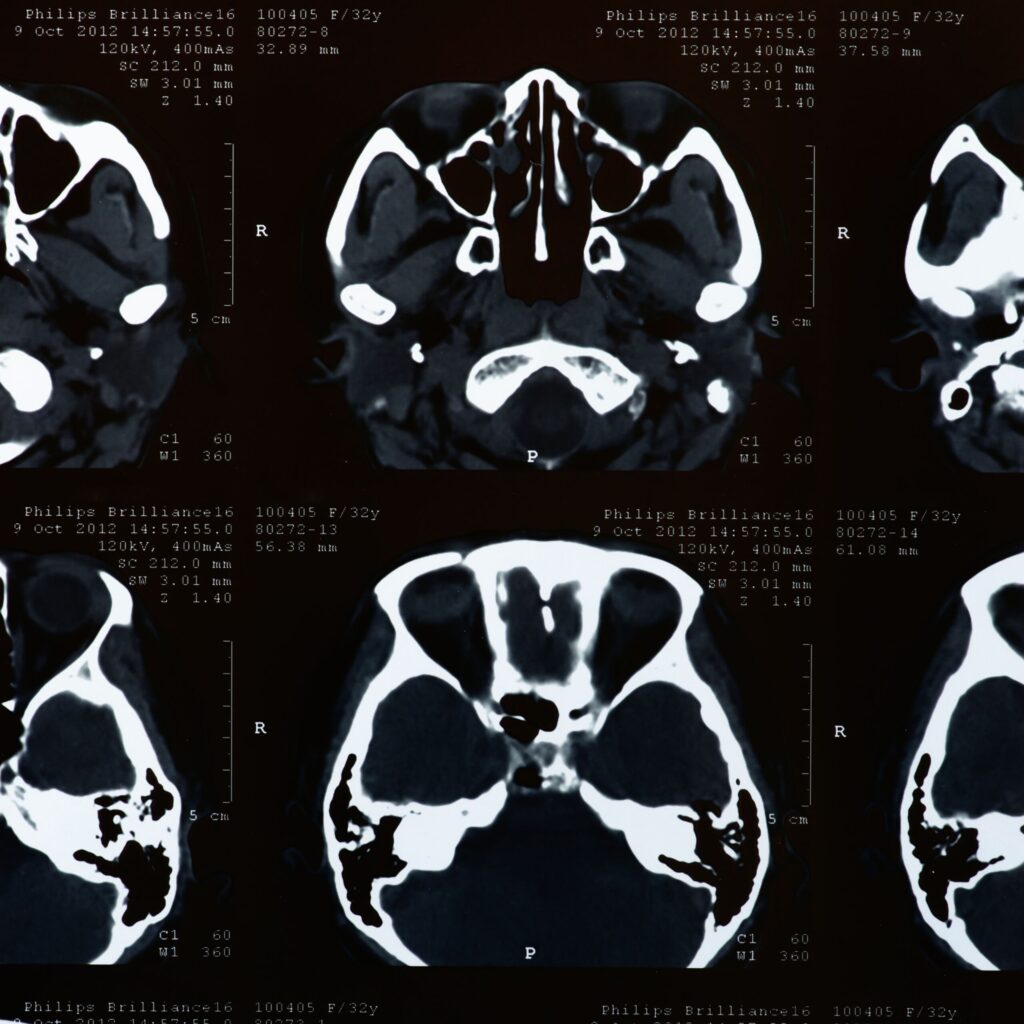
The case demonstrates that acute ischaemic stroke is a time-critical emergency. Medical negligence occurs far too often when FAST-positive symptoms (face, arm, speech, time) are not treated as such in A&E. National guidelines require immediate CT head within 20 minutes of arrival and thrombolysis within 60 minutes (door-to-needle) or thrombectomy within 6–24 hours in eligible cases.
The delay in this case highlights the need for mandatory stroke training for all A&E staff, clear stroke pathways with rapid senior review, and a low threshold for activating the stroke team. Medical negligence can be prevented through consistent application of the FAST test, rapid imaging and treatment protocols.
Patient safety organisations continue to campaign for better implementation of hyperacute stroke pathways and 24/7 access to thrombectomy centres. Medical negligence in failing to treat stroke promptly can lead to massive, preventable disability — an outcome that could have been largely avoided with timely intervention.
Support and Advice for Stroke Victims
If you or a loved one has suffered severe disability or death after a suspected delayed stroke diagnosis or treatment caused by medical negligence, early specialist legal advice is essential. Time limits apply (usually three years from awareness of harm caused by medical negligence, or from date of death), but acting promptly preserves evidence and allows access to support services.
Specialist medical negligence solicitors assess cases on a No-Win-No-Fee basis after initial review. They instruct leading stroke physicians, neurologists and neuroradiologists to prove medical negligence and secure maximum compensation for lifelong needs after preventable stroke injury.
The family hopes this case raises awareness of the urgency required in stroke care. Medical negligence in failing to activate the stroke pathway promptly can have catastrophic consequences. Immediate CT scanning, thrombolysis and thrombectomy remain the key to preventing avoidable disability and death.
Categories: Medical Negligence, Stroke, Delayed Diagnosis, Patient Safety
Keywords: stroke misdiagnosis, medical negligence delayed thrombolysis, A&E stroke failure, preventable hemiplegia, ischaemic stroke negligence, hyperacute stroke protocol breach, NHS stroke care failings
 English
English